Targeted prevention measures and process hygiene in veterinary medicine
Prevention of infections and sepsis caused by intravascular catheters in veterinary medicine (ICRI and CABSI)
The aim of all hygiene measures is to reduce nosocomial infections and protect employees from occupational infections. In order to keep the infection rate as low as possible, you should consider and optimize the entire process and develop bundle strategies.
Focus topic
Intravascular catheter-related infections
Infections and sepsis caused by intravascular catheters in veterinary medicine (ICRI – Intravascular Catheter-Related Infections and CABSI – Catheter-Associated Blood Stream Infections)
Infusion Therapy
Infusion therapy
Handling infusion solutions: The preparation of infusion solutions is an aseptic activity. The work surface must be disinfected and hygienic hand disinfection (e.g., SoftaMan® pure) must be carried out. When priming the infusion line, ensure that the attachment is not contaminated. Infusion systems with Primestops (e.g., Intrafix® SafeSet) help with this, as the protective cap of the infusion line does not have to be removed for priming. Another advantage of systems such as the Intrafix® SafeSet is that the system does not run empty thanks to the AirStop filter. This can reduce the number of disconnections and thus reduce the risk of bacterial contamination of the catheter. Since disconnection of the patient’s infusion solutions must be performed much more frequently in veterinary medicine than in human medicine, the recommendations here are only to be applied to a limited extent. But this is precisely why thorough basic and hand hygiene is crucial for prevention.

For each disconnection, the infusion line must be closed with a fresh, sterile seal plug and the Luer lock connector must be disinfected with a spray disinfectant (e.g., Softasept® N) before reconnecting.
The use of infusion systems that work without ventilation (Ecoflac®) also appears to have a positive effect on the reduction of infections. [1]
In-line filters (bacteria and particulate filters such as Sterifix®) are able to prevent severe complications in intensive care patients, such as the occurrence of SIRS, and should therefore be used for the infusion therapy of critically ill and intensive-care. [2-4]
Step-by-step guide

Service life of infusion systems: The change intervals for infusion systems are about 96 hours. Three-way stopcock and needle-free connection systems are also included here. Infusion systems through which lipid solutions are led should be changed every 24 hours. Blood product transfusion systems must be changed every 6 hours. The entire system should be replaced in the event of contamination of a system or indications of CRBSI. [3-5]
Appropriate products





Prevention of Vascular Catheter-Associated Infections and Primary Sepsis
Prevention of vascular catheter-associated infections and primary sepsis
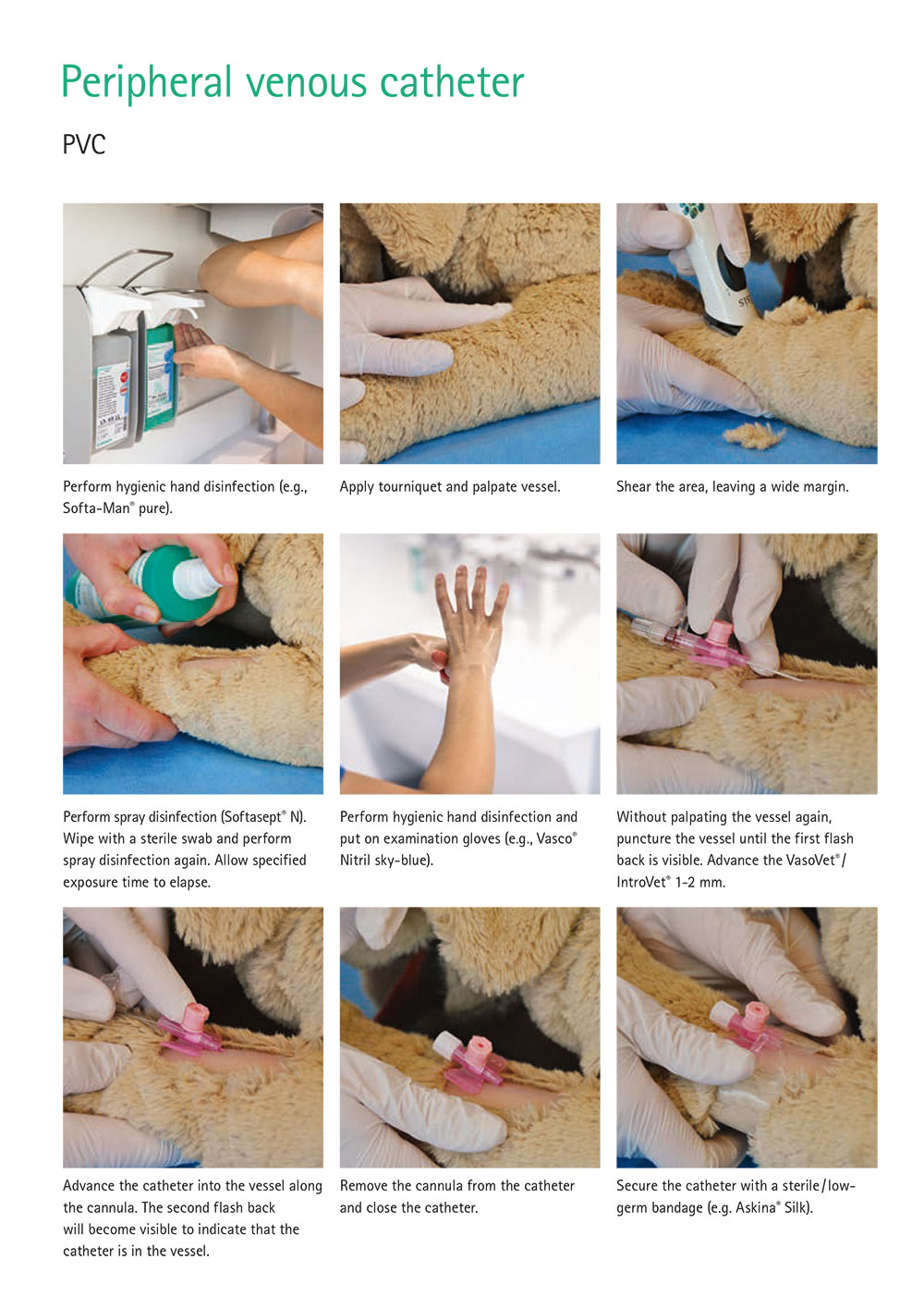
Puncturing of veins and placement of peripheral venous catheters
Placement: The vein should always be congested and palpated before shearing. If there are signs of phlebitis or local skin inflammation, a different site should be chosen. The puncture site must be shorn over a large area. Puncture of veins or placement of an intravenous catheter is an aseptic activity. Therefore, the work surface must be disinfected and hygienic hand disinfection carried out. In a prospective study in human medicine, the risk of AIF-associated complications decreased significantly after hand disinfection, while hand washing had no influence on the complication rate. [5] The puncture site should then be disinfected. This can be done by spraying or wiping with an alcohol-based antiseptic (e.g., Softasept® N). It is important to observe the contact time.
For occupational health and safety reasons, low-germ disposable gloves should be used. Avoid re-palpation of the vessel after disinfection. Puncture the vessel and advance the catheter into the vessel, ensuring that the catheter does not touch the fur (Left Step by Step PVC). The catheter is then fixed and flushed.
As venous catheter placement is an invasive procedure, it must be recorded in the patient’s veterinary record along with the date. Catheter changes should be performed within 24 hours [5, 6] for catheters in which asepsis has not been observed, e.g., in emergency situations.

Material: Several studies have shown the advantage of polyurethane (PUR) and teflon over other materials in terms of phlebitis. [7] B. Braun catheters such as VasoVet®, IntroVet® and Braunüle® Vet High Flow, for example, are made of PUR.
Care: Sanitary hand disinfection must be carried out prior to every manipulation. The indication for an AIF should be checked daily. Catheters that are no longer needed should be removed. The dressing should be changed daily and the puncture site checked for signs of infection/phlebitis. We recommend using an extension with a needle-free diaphragm valve (CareSite®). The smooth surface of the CareSite® can be easily disinfected by spraying or wiping prior to drug application and also reduces manipulation of the catheter itself. In turn, this can also reduce any mechanical irritation of the vein wall and avoid the risk of contamination of the catheter hub. When disconnected, the positive pressure in the CareSite® valve prevents blood from entering and coagulating the catheter. The use of T-connectors is not recommended as they are associated with a higher risk of contamination compared to Y-connectors such as the CareSite®. [8]
Recommendation

Replacement intervals of infusion systems
A recommendation of the Commission for Hospital Hygiene and Infection Prevention (KRINKO) at the Robert Koch Institute (RKI)
Dwelling time: There are barely any studies in veterinary medicine on this subject. It can be assumed that due to the high number of complications (mechanical and inflammatory) and generally poor hand hygiene, statements on this should be considered carefully. One study found the best time to change the catheter to be 36 hours [9] while other authors indicate up to 72 hours. Although the colonization rate increases over time, this does not appear to have an effect on the infection rate compared to catheters that dwell for 96 hours. [10] With hygienic handling and good management, there is no need for routine changes. Alternatively, an interval should be defined according to your own risk analysis. [6]
In any case, the catheter and the infusion set must be changed if there are signs of phlebitis. [6, 11]
Training sessions: Good training for the placement of venous catheters is one of the basic requirements for preventing catheter infections.
Step-by-step guide
Central venous catheter (CVC)
Placement: First, hygienic hand disinfection is carried out before the work surface is disinfected and sterilely covered. The puncture site is sheared over a large area and prepared as is the case for a surgical procedure. We recommend pre-cleaning the skin with a polyhexanide foam. This removes dirt, sebum, and microorganisms. After one minute of exposure, the area can be dried with a clean swab. This is followed by a 2-phase disinfection. The area is treated with sterile swabs (e.g., Askina® Sling Gauze Swabs) soaked in disinfectant (e.g., Braunoderm®) plus the use of grain forceps (e.g., Aesculap® grain forceps) or treated using a spray disinfection (e.g., Braunoderm®). The vet should carry out any preparation as they would for any surgery, i.e., put on a face mask and hood, perform surgical hand disinfection (e.g., with Promanum® pure) and don a sterile gown and gloves (e.g., Vasco® OP Grip). The patient is sterilely covered, and the catheter (e.g., Certofix®) is inserted and fixed. The puncture site is cleaned (Prontovet® Solution). A polyhexanide wound gel (e.g., ProntoVet® Gel) is then applied to the puncture site. The catheter is then protected with a sterile compress and a bandage.

Care: Hygienic hand disinfection (e.g., SoftaMan® pure) must be carried out before each and every manipulation. The connection valves, the three-way stopcock, or the hub must be disinfected before each administration of medication or connection. The bandage should be changed at least every 72 hours or when it gets soiled. The puncture site, together with any residual active agent, should be cleaned with alcohol (Softasept® N and ProntoVet®) and wetted with an antiseptic wound gel (ProntoVet® Gel). Manipulation of the catheter hub and the three-way stopcock can lead to massive contamination of the catheter. Studies have shown a rate of up to 20 percent. [12-16]
The use of needle-free connector valves (CareSite®) can reduce the contamination rate. [17-19] The prerequisite for this is that the personnel are familiarized with the product and trained in its use before the needle-free connection valve is introduced.
The positive pressure valves appear to be superior after 7 days of use than neutral or negative pressure valves (CareSite® is a positive pressure valve!). [17, 20] Sterile 0.9 percent saline is used for flushing catheters. [21]
Contact/dwelling time: Indications should be checked daily. If evidence of phlebitis and inflammation at the site of injection are observed, the CVC must be removed.
Training sessions: Personnel must be regularly and extensively trained in the use of CVCs.
Step-by-step guide

Appropriate products











Drug Preparation
Drug preparation
Contamination may occur during the preparation or reconstruction (preparation for use) of drugs, drawing up of drugs, or preparation of infusion solutions. These can, in turn, lead to catheter-associated infections or infections at the injection site.
Before each preparation and reconstruction, disinfect the work surface (e.g., with Meliseptol® acute) and disinfect your hands (e.g., with Softa-Man® pure).
Aseptic drawing must be ensured. The rubber plug must be disinfected before drawing. The use of a B. Braun Mini-Spike® / Minispike® 2 is recommended for multi-dose containers. [22]
Step-by-step guide

Appropriate products








[1] Maki DG, Rosenthal VD, Salomao R, Franzetti F, Rangel-Frausto MS. Impact of switching from an open to a closed infusion system on rates of central line-associated bloodstream infection: a meta-analysis of time-sequence cohort studies in 4 countries. Infect Control Hosp Epidemiol 2011; 32(1):50 8.
[2] Jack T, Boehne M, Brent BE, Hoy L, Köditz H, Wessel A et al. In-line filtration reduces severe complications and length of stay on pediatric intensive care unit: a prospective, randomized, controlled trial. Intensive care medicine 2012; 38(6):1008 16.
[3] Prävention von Infektionen, die von Gefäßkathetern ausgehen (Prevention of infections from vascular catheters): Hinweise zur Implementierung Informativer Anhang 2 zur Empfehlung der Kommission für Krankenhaushygiene und Infektionsprävention (KRINKO) beim Robert Koch-Institut (Notes on the implementation of informative Annex 2 to the recommendation of the Commission for Hospital Hygiene and Infection Prevention (KRINKO) at the Robert Koch Institute). Bundesgesundheitsbl 2017; 60(2):231-44.
[4] Prävention von Infektionen, die von Gefäßkathetern ausgehen (Prevention of infections from vascular catheters): Teil 1 – Nichtgetunnelte zentralvenöse Katheter Empfehlung der Kommission für Krankenhaushygiene und Infektionsprävention (KRINKO) beim Robert Koch-Institut (Part 1 – Non-tunneled central venous catheters. Recommendation of the Commission for Hospital Hygiene and Infection Prevention (KRINKO) at the Robert Koch Institute). Bundesgesundheitsbl 2017; 60(2):171-206.
[5] Department of Health and Human Services, Centers for Disease Control and Prevention. Guidelines for the Prevention of Intravascular Catheter-Related Infections (2011).
[6] Prävention von Infektionen, die von Gefäßkathetern ausgehen (Prevention of infections from vascular catheters): Teil 2 – Periphervenöse Verweilkanülen und arterielle Katheter Empfehlung der Kommission für Krankenhaushygiene und Infektionsprävention (KRINKO) beim Robert Koch-Institut (Part 2 – Periphervenous indwelling cannulae and arterial catheters. Recommendation of the Commission for Hospital Hygiene and Infection Prevention (KRINKO) at the Robert Koch Institute). Bundesgesundheitsbl 2017; 60(2):207-15.
[7] Müller C, Gehlen H. Katheterassoziierte Venenerkrankungen beim Pferd - Diagnose und Therapie in der Praxis (Catheter-associated venous disease in horses – diagnosis and therapy in practice). Tierarztl Prax Ausg G Grosstiere Nutztiere 2016; 44(3):187-94.
[8] Jones ID, Case AM, Stevens KB, Boag A, Rycroft AN. Factors contributing to the contamination of peripheral intravenous catheters in dogs and cats. Vet Rec 2009; 164(20):616-8.
[9] Crisi PE, Santis F de, Aste G, Tiscar PG, Mosca F, Gasparini A et al. Inflammatory, Mechanical and Infectious Complications Associated with Peripheral Intravenous Catheters in Dogs and Cats: A Risk Factor Analysis. Vet Sci 2022; 9(3).
[10] Lai KK. Safety of prolonging peripheral cannula and i.v. tubing use from 72 hours to 96 hours. Am J Infect Control 1998; 26(1):66-70.
[11] Naomi P. O'Grady, M.D.1, Mary Alexander, R.N.2, Lillian A. Burns, M.T., M.P.H., C.I.C.3, E. Patchen Dellinger, M.D.4, Jeffery Garland, M.D., S.M.5, Stephen O. Heard, M.D.6, Pamela A. Lipsett, M.D.7, Henry Masur, M.D.1, Leonard A. Mermel, D.O., Sc.M.8, Michele L. Pearson, M.D.9, Issam I. Raad, M.D.10, Adrienne Randolph, M.D., M.Sc.11, Mark E. Rupp, M.D.12, Sanjay Saint, M.D., M.P.H. Guidelines for the Prevention of Intravascular Catheter-Related Infections, 2011 2017.
[12] Oto J, Nishimura M, Morimatsu H, Katayama H, Onodera M, Takahashi H et al. Comparison of contamination between conventional three-way stopcock and needleless injection device: a randomized controlled trial. Med Sci Monit 2007; 13(10):CR417-21.
[13] Sitges-Serra A, Puig P, Liñares J, Pérez JL, Farreró N, Jaurrieta E et al. Hub colonization as the initial step in an outbreak of catheter-related sepsis due to coagulase negative staphylococci during parenteral nutrition. JPEN J Parenter Enteral Nutr 1984; 8(6):668-72.
[14] Sitges-Serra A, Hernández R, Maestro S, Pi-Suñer T, Garcés JM, Segura M. Prevention of catheter sepsis: the hub. Nutrition 1997; 13(4 Suppl):30S-35S.
[15] Lockman JL, Heitmiller ES, Ascenzi JA, Berkowitz I. Scrub the hub! Catheter needleless port decontamination. Anesthesiology 2011; 114(4):958.
[16] Liñares J, Sitges-Serra A, Garau J, Pérez JL, Martín R. Pathogenesis of catheter sepsis: a prospective study with quantitative and semiquantitative cultures of catheter hub and segments. J Clin Microbiol 1985; 21(3):357-60.
[17] Costello JM, Morrow DF, Graham DA, Potter-Bynoe G, Sandora TJ, Laussen PC. Systematic intervention to reduce central line-associated bloodstream infection rates in a pediatric cardiac intensive care unit. Pediatrics 2008; 121(5):915-23.
[18] Yébenes JC, Vidaur L, Serra-Prat M, Sirvent JM, Batlle J, Motje M et al. Prevention of catheter-related bloodstream infection in critically ill patients using a disinfectable, needle-free connector: a randomized controlled trial. Am J Infect Control 2004; 32(5):291-5.
[19] Bouza E, Muñoz P, López-Rodríguez J, Jesús Pérez M, Rincón C, Martín Rabadán P et al. A needleless closed system device (CLAVE) protects from intravascular catheter tip and hub colonization: a prospective randomized study. J Hosp Infect 2003; 54(4):279-87.
[20] Harnage S. Seven years of zero central-line-associated bloodstream infections. Br J Nurs 2012; 21(21):S6, S8, S10-2.
[21] Vose J, Odunayo A, Price JM, Daves M, Schildt JC, Tolbert MK. Comparison of heparinized saline and 0.9% sodium chloride for maintaining central venous catheter patency in healthy dogs. PeerJ 2019; 7:e7072.
[22] Popp W. und Zastrow K-D. Hygiene-Tipp, Dezember 2008 Deutsche Gesellschaft für Krankenhaushygiene: Einzeldosisampullen oder Mehrdosenbehältnisse für Injektionen.